Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services
Coverage Period: 01/01/2021 - 12/31/2021
Horizon BCBSNJ: State Health Benefits Program- NJ DIRECT (PPO)
Coverage for: All Coverage Types
Plan Type: PPO
(NJ DIRECT (PPO))/BlueCard
1 of 9
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the
plan would share the cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will
be provided separately. This is only a summary. Benefits may change upon renewal. For more information about your coverage, or to get a
copy of the complete terms of coverage, visit Member Online Services at http://www.nj.gov/treasury/pensions/index.shtml or by calling 1-609-
292-7524. If you do not currently have coverage with Horizon BCBSNJ you can view a sample policy here,
http://www.nj.gov/treasury/pensions/index.shtml. For general definitions of common terms, such as allowed amount, balance billing,
coinsurance, copayment, deductible, provider, or other underlined terms see the Glossary. You can view the Glossary at www.cciio.cms.gov or
call 1-609-292-7524 to request a copy.
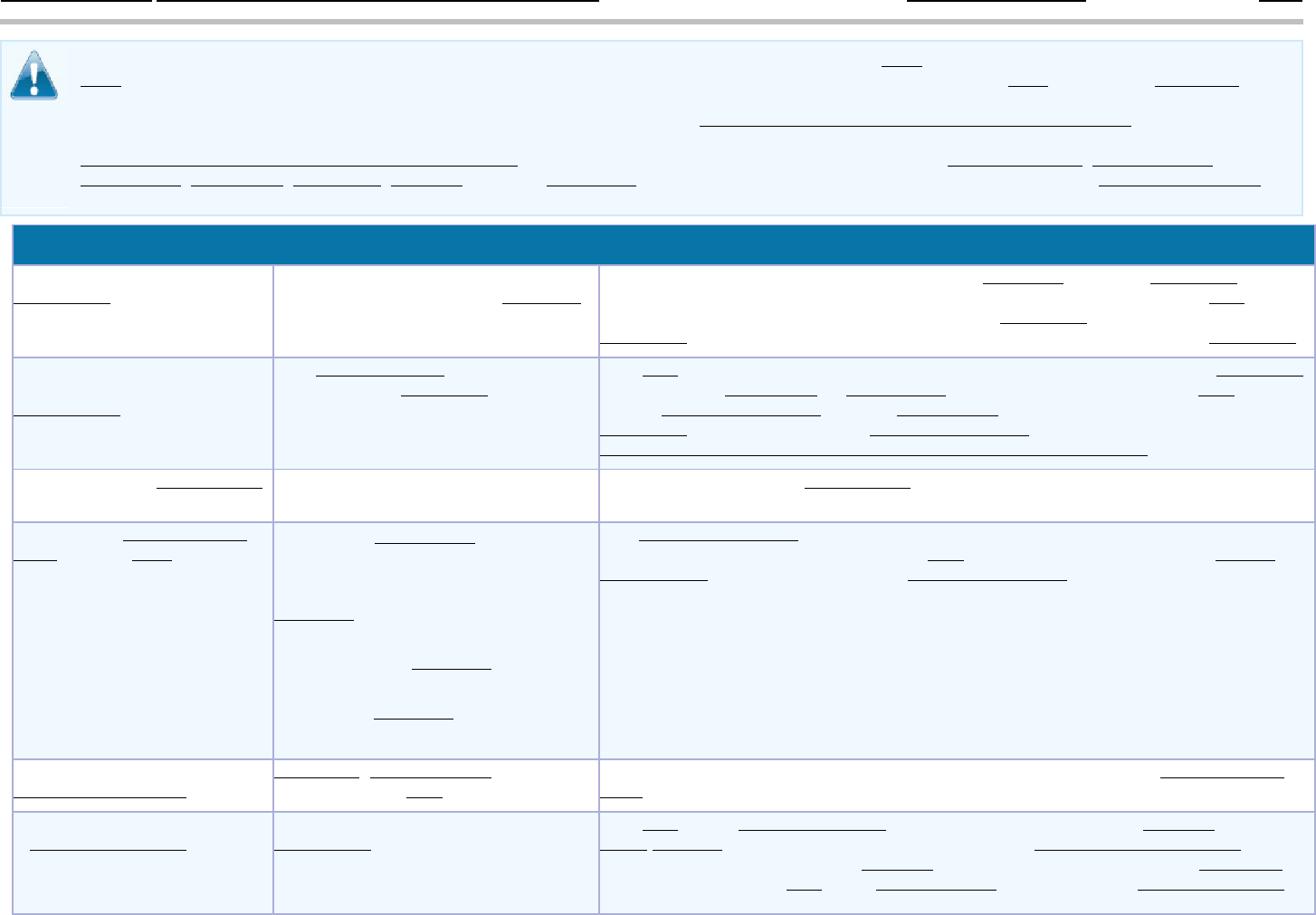
Important Questions
Answers
Why This Matters:
What is the overall
deductible
?
$400.00 Individual / $1,000.00
Family for out-of-network providers.
Aggregate family.
Generally, you must pay all of the costs from providers up to the deductible amount
before this plan begins to pay. If you have other family members on the
plan, each
family member must meet their own individual
deductible until the total amount of
deductible
expenses paid by all family members meets the overall family deductible.
Are there services covered
before you meet your
deductible
?
Yes. Preventive care is covered before
you meet your deductible.
This plan covers some items and services even if you haven’t yet met the deductible
amount. But a
copayment or coinsurance may apply. For example, this plan covers
certain
preventive services without cost-sharing and before you meet your
deductible
. See a list of covered preventive services at
https://www.healthcare.gov/coverage/preventive
-care-benefits/.
Are there other deductibles
for specific services?
No.
You don’t have to meet deductibles for specific services.
What is the out-of-pocket
limit
for this plan?
In-network coinsurance limit $800.00
Individual/$2,000.00 Family; Active
employee in-network Health
providers $6,840.00 Individual/
$13,680.00 Family. Retiree in-
network Health providers $7,199.00
Individual/$14,398.00 Family. Out-
of-network providers $2,000.00
Individual/$5,000.00 Family.
The out-of-pocket limit is the most you could pay in a year for covered services. If
you have other family members in this
plan, they have to meet their own out-of-
pocket limits
until the overall family out-of-pocket limit has been met.
What is not included in the
out
-of-pocket limit?
Premiums, balance-billing charges and
health care this plan doesn’t cover.
Even though you pay these expenses, they don’t count toward the out-of-pocket
limit
.
Will you pay less if you use
a
network provider?
Yes. For a list of in-network
providers, see
www.HorizonBlue.com/shbp or
call 1-800-414-SHBP (7427).
This plan uses a provider network. You will pay less if you use a provider in the
plan's
network. You will pay the most if you use an out-of-network provider, and
you might receive a bill from a
provider for the difference between the provider's
charge and what your
plan pays (balance billing). Be aware your network provider
* For more information about limitations and exceptions, see the plan or policy document at
http://www.nj.gov/treasury/pensions/index.shtml
2 of 9
might use an out-of-network provider for some services (such as lab work). Check
with your
provider before you get services.
Do you need a referral to
see a specialist?
No.
You can see the specialist you choose without a referral.
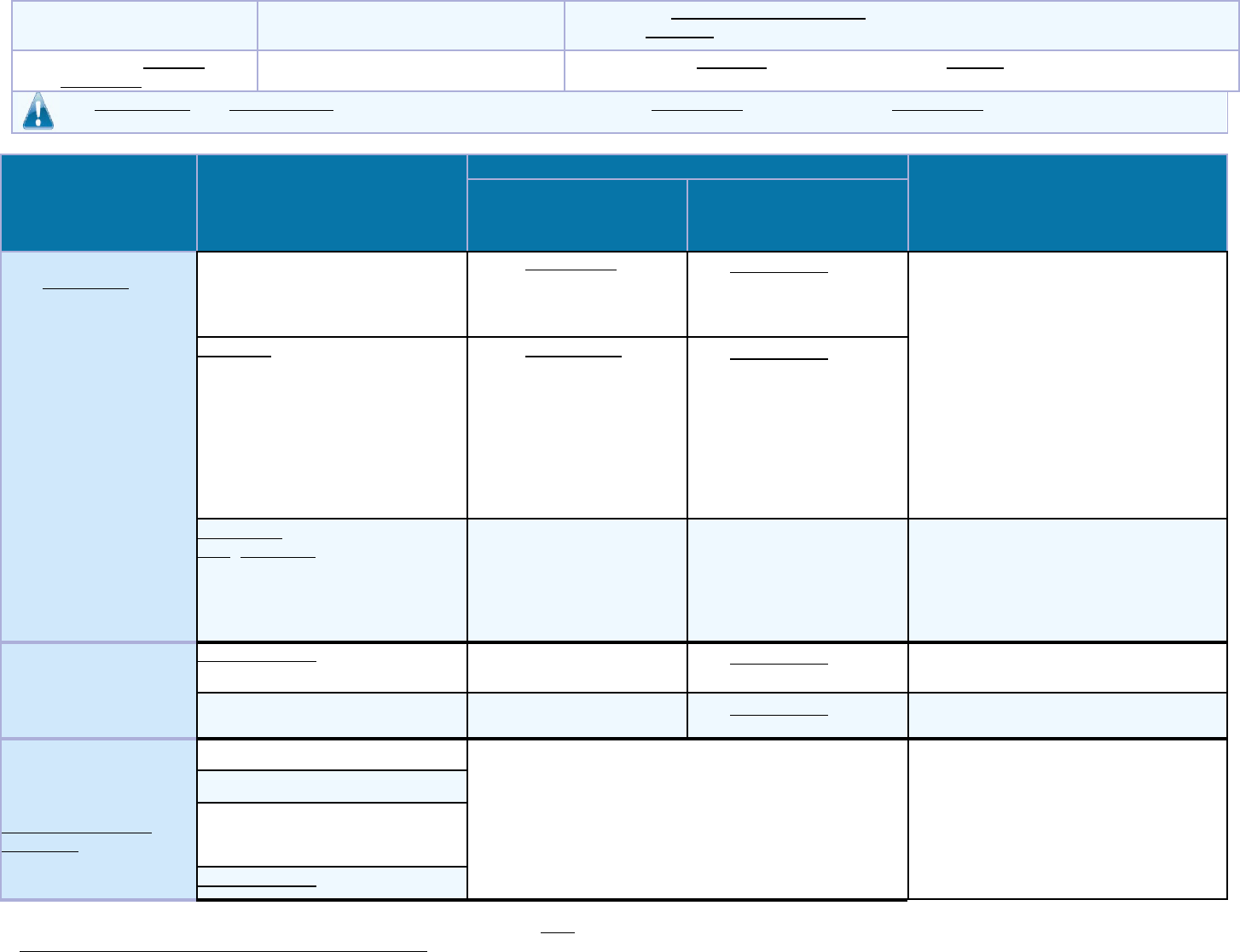
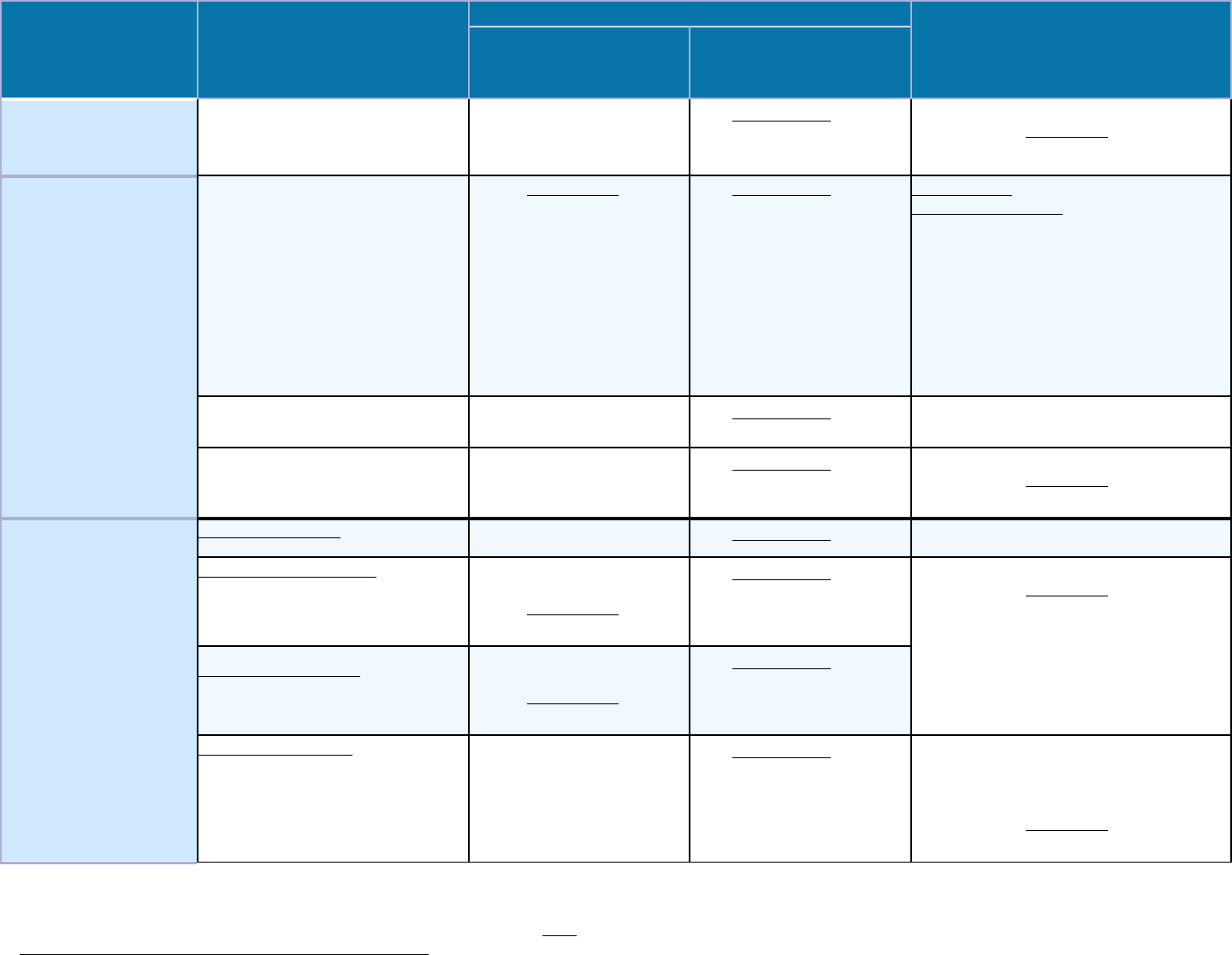
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical Event
Services You May Need
What You Will Pay
Limitations, Exceptions, & Other
Important Information
Network Provider
(You will pay the
least)
Out-of-Network
Provider(You will pay
the most)
If you visit a health
care
provider’s office
or clinic
Primary care visit to treat an
injury or illness
$15.00 Copayment per
visit
.
30% Coinsurance.
Out-of-network reimbursement is
based on 175% of CMS, except where
noted. Out
-of-network coverage for
Chiropractic, acupuncture and
physical
therapy services are limited to no more
than $35 a visit for chiropractic and $60
a visit for acupuncture and $52 a visit
for physical therapy or 75% of the in
network cost per visit, whichever is
less.
Specialist visit
$15.00 Copayment per
visit
.
30% Coinsurance.
Preventive
care
/screening/immunization
No Charge.
Not Covered.
One per calendar year. You may have
to pay for se
rvices that aren't
preventive.
Ask your provider if the
services needed are pre
ventive. Then
check what your plan will pay for.
If you have a test
Diagnostic test (x-ray, blood
work)
No Charge.
30% Coinsurance.
__________
none
__________
Imaging (CT/PET scans, MRIs)
No Charge.
30% Coinsurance.
Requires pre-approval.
If you need drugs to
treat your illness or
condition
More information about
prescription drug
coverage
is available
through your employer.
Generic drugs
See separate Prescription Drug Plan SBC
__________
none
__________
Preferred brand drugs
Non-preferred brand drugs
Specialty drugs
* For more information about limitations and exceptions, see the plan or policy document at
http://www.nj.gov/treasury/pensions/index.shtml
3 of 9
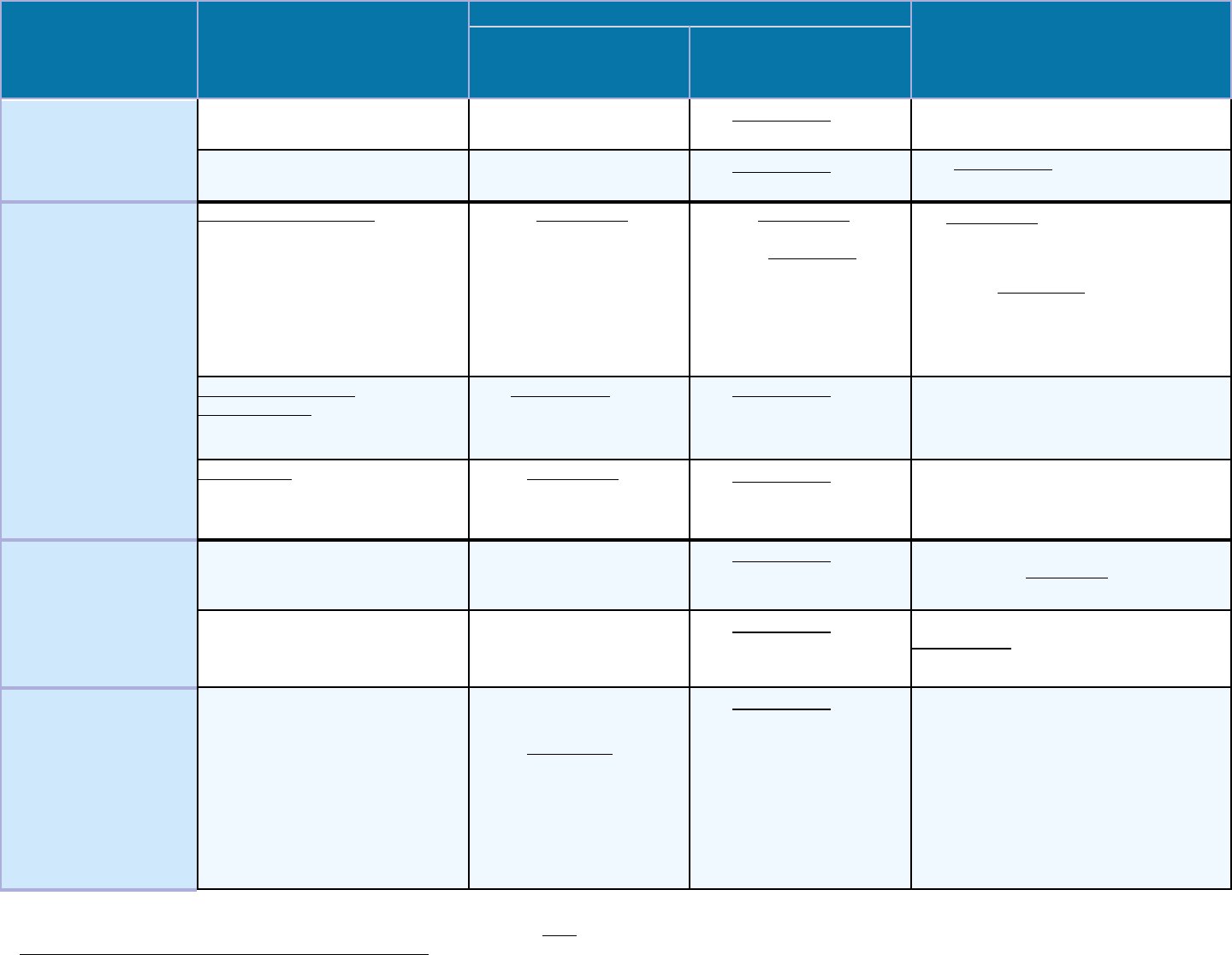
Common
Medical Event
Services You May Need
What You Will Pay
Limitations, Exceptions, & Other
Important Information
Network Provider
(You will pay the
least)
Out-of-Network
Provider(You will pay
the most)
If you have
outpatient surgery
Facility fee (e.g., ambulatory
surgery center)
No Charge.
30% Coinsurance.
__________
none
__________
Physician/surgeon fees
No Charge.
30% Coinsurance.
30% Coinsurance for out-of-network
anesthesia.
If you need
immediate medical
attention
Emergency room care
$150.00 Copayment per
visit
for Outpatient
Hospital.
$150.00 Copayment per
visit for Outpatient
Hospital. Deductible does
not apply.
$50 Copayment/visit for physician
referrals
and pediatric (under age 19)
ER visits; and if admitted within 24
hours, the
copayment is waived.
Payment at the in
-
network level applies
only to true Medical Emergencies &
Accidental Injuries.
Emergency medical
transportation
10% Coinsurance.
30% Coinsurance.
Limited to local emergency transport to
the nearest facility equipped to treat the
emergency
condition.
Urgent care
$15.00 Copayment per
visit
.
30% Coinsurance.
__________
none
__________
If you have a
hospital stay
Facility fee (e.g., hospital room)
No Charge.
30% Coinsurance.
Requires pre-approval. There is a
separate $5
00 deductible per inpatient
stay for out
-of-network facilities.
Physician/surgeon fees
No Charge.
30% Coinsurance.
Requires pre-approval. 30%
Coinsurance
for out-of-network
anesthesia.
If you need mental
health, behavioral
health, or substance
abuse services
Outpatient services
No Charge for Outpatient
Hospital.
$15.00
Copayment per
O
ffice visit for Mental
Health and Behavioral
Health.
No Charge for
Substance Abuse O
ffice
visit.
30% Coinsurance.
Some specialty outpatient services
require pre
-approval. Mental health
services will be reimbursed at 175% of
CMS
fee schedule up to reaching the
Maximum out
-of-pocket (MOOP) of
$2,000 (individual) or $5,000 (
family).
Once
MOOP has been met
services
will be reimbursed at 195% of
CMS
fee schedule for the remainder of
the
plan year.
* For more information about limitations and exceptions, see the plan or policy document at
http://www.nj.gov/treasury/pensions/index.shtml
4 of 9
Common
Medical Event
Services You May Need
What You Will Pay
Limitations, Exceptions, & Other
Important Information
Network Provider
(You will pay the
least)
Out-of-Network
Provider(You will pay
the most)
Inpatient services
No Charge.
30% Coinsurance.
Requires pre-approval. There is a
separate $5
00 deductible per inpatient
stay for out
-of-network facilities.
If you are pregnant
Office visits
$15.00 Copayment per visit
for Office.
30% Coinsurance.
Cost sharing does not apply for
preventive services
. Maternity care may
include tests and services descri
bed
elsewher
e in the SBC (i.e. Ultrasound.).
OON obstetrics services
with a date of
service prior to 7/1/19 will be
reimbursed at 195% of CMS fee
schedule. OON obstetrics services with
a date of service on or after 7/1/19
will
be reimbursed at 175% of CMS
fee
schedule.
Childbirth/delivery professional
services
No Charge.
30% Coinsurance.
__________
none
__________
Childbirth/delivery facility
services
No Charge.
30% Coinsurance.
Requires pre-approval. There is a
separate
$500 deductible per inpatient
stay for out
-of-network facilities.
If you need help
recovering or have
other special health
needs
Home health care
No Charge.
30% Coinsurance.
Requires pre-approval.
Rehabilitation services
No Charge for Inpatient
and Outpatient Facility.
$1
5.00 Copayment per visit
for Office.
30% Coinsurance.
Requires pre-approval. There is a
separate $5
00 deductible per inpatient
stay for out
-of-network facilities.
Habilitation services
No Charge for Inpatient
and Outpatient Facility.
$1
5.00 Copayment per visit
for Office.
30% Coinsurance.
Skilled nursing care
No Charge.
30% Coinsurance.
Requires pre-approval. Limited to 120
days in
-network and 60 out-of-
network
facility days for a combined maximum
of 120 days per calendar year.
There is a
separate $5
00 deductible per inpatient
stay for out
-of-network facilities.
* For more information about limitations and exceptions, see the plan or policy document at
http://www.nj.gov/treasury/pensions/index.shtml
5 of 9
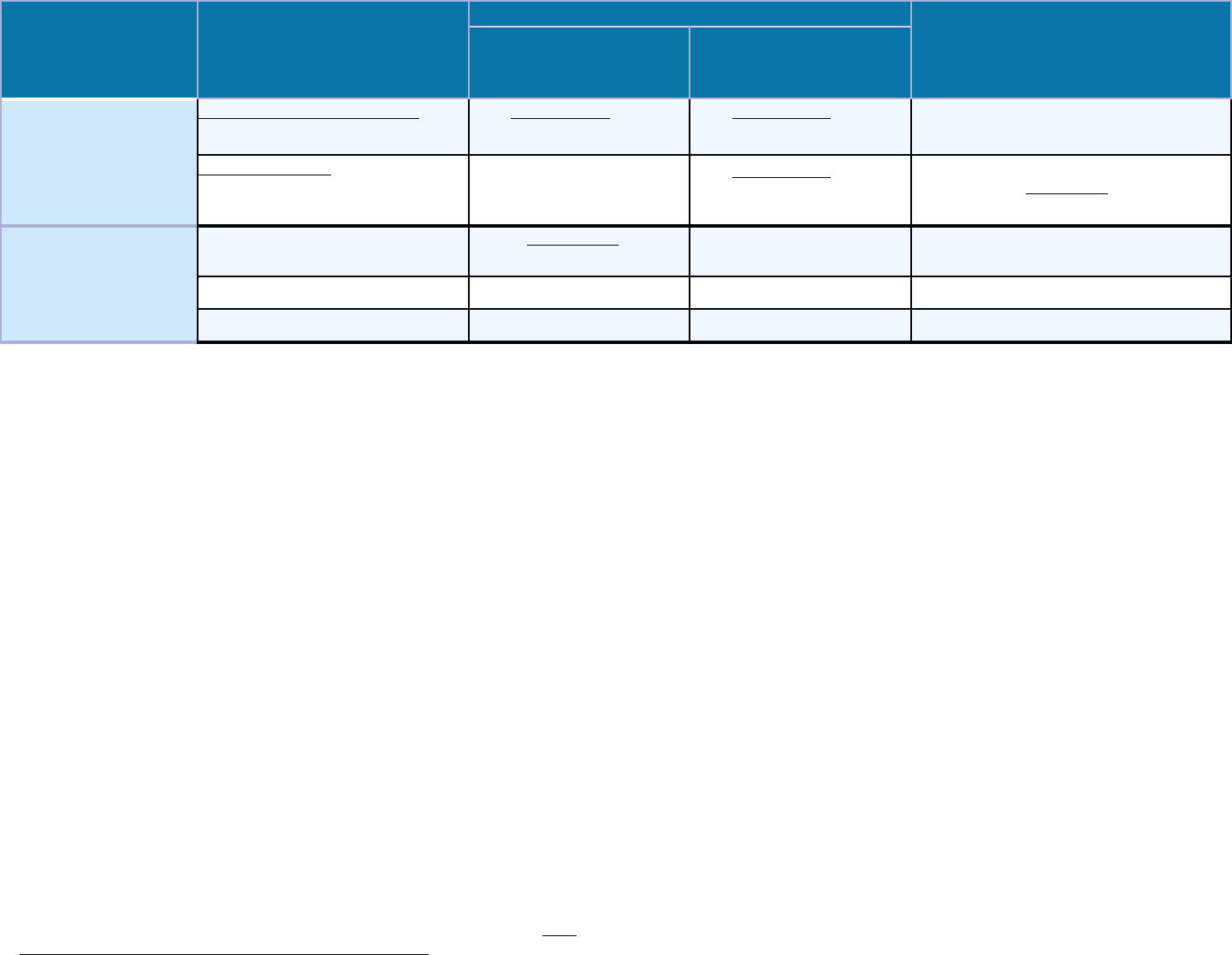
Common
Medical Event
Services You May Need
What You Will Pay
Limitations, Exceptions, & Other
Important Information
Network Provider
(You will pay the
least)
Out-of-Network
Provider(You will pay
the most)
Durable medical equipment
10% Coinsurance.
30% Coinsurance.
Requires pre-approval for all rentals
and some purchases.
Hospice services
No Charge.
30% Coinsurance.
Requires pre-approval. There is a
separate $5
00 deductible per inpatient
stay for out
-of-network facilities.
If your child needs
dental or eye care
Children’s eye exam
$15.00 Copayment per
visit
.
Not Covered.
Coverage is limited to 1 visit.
Children’s glasses
Not Covered.
Not Covered.
__________
none
__________
Children’s dental check-up
Not Covered.
Not Covered.
__________
none
__________
* For more information about limitations and exceptions, see the plan or policy document at
http://www.nj.gov/treasury/pensions/index.shtml
6 of 9
Excluded Services & Other Covered Services:
Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded
services.)
●
Cosmetic Surgery
●
Dental care (Adult)
●
Long Term Care
●
Private-duty nursing
●
Routine foot care
●
Weight Loss Programs
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)
●
Acupuncture (for pain management only)
●
Bariatric surgery (requires pre-approval)
●
Chiropractic care (limited to 30 visits/year)
●
Hearing Aids (Only covered for members age
15 or younger)
●
Infertility treatment (requires pre-approval)
●
Most coverage provided outside the United
States.
(Subject to deductible/coinsurance
and balance billing.)
●
Non-emergency care when traveling outside
the U.S. (
Subject to deductible/coinsurance
and balance billing.)
●
Routine eye care (Adult)
* For more information about limitations and exceptions, see the plan or policy document at
http://www.nj.gov/treasury/pensions/index.shtml
7 of 9
Your Rights to Continue Coverage:
There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agencies is: the plan at 1-800-414-
7427 (SHBP), the Department of Health and Human Services, Center for Consumer Information and Insurance Oversight, at 1-877-267-
2323 x61565 or
www.cciio.cms.gov, or the U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa. Other
coverage options may be available to you, too, including buying individual insurance coverage through the Health Insurance Marketplace. For more
information about the Marketplace, visit www.getcovered.nj.gov or call 1-877-962-8448.
Your Grievance and Appeals Rights:
There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance or appeal. For more
information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide complete
information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance,
contact: Horizon Blue Cross Blue Shield of New Jersey Member Services at 1-800-414-SHBP (7427). You may also contact the Department of Labor’s
Employee Benefits Security Administration at 1-866-444-EBSA (3272) or www.dol.gov/ebda/healthreform.
Does this plan provide Minimum Essential Coverage? Yes
Minimum Essential Coverage generally includes plans, health insurance available through the Marketplace or other individual market policies, Medicare,
Medicaid, CHIP, TRICARE, and certain other coverage. If you are eligible for certain types of Minimum Essential Coverage, you may not be eligible for the
premium tax credit.
Does this plan meet the Minimum Value Standards? Yes
If your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the
Marketplace.
-----------------------------------------To see examples of how this plan might cover costs for a sample medical situation, see the next section.---------------------------------------------
* For more information about limitations and exceptions, see the plan or policy document at
http://www.nj.gov/treasury/pensions/index.shtml
8 of 9
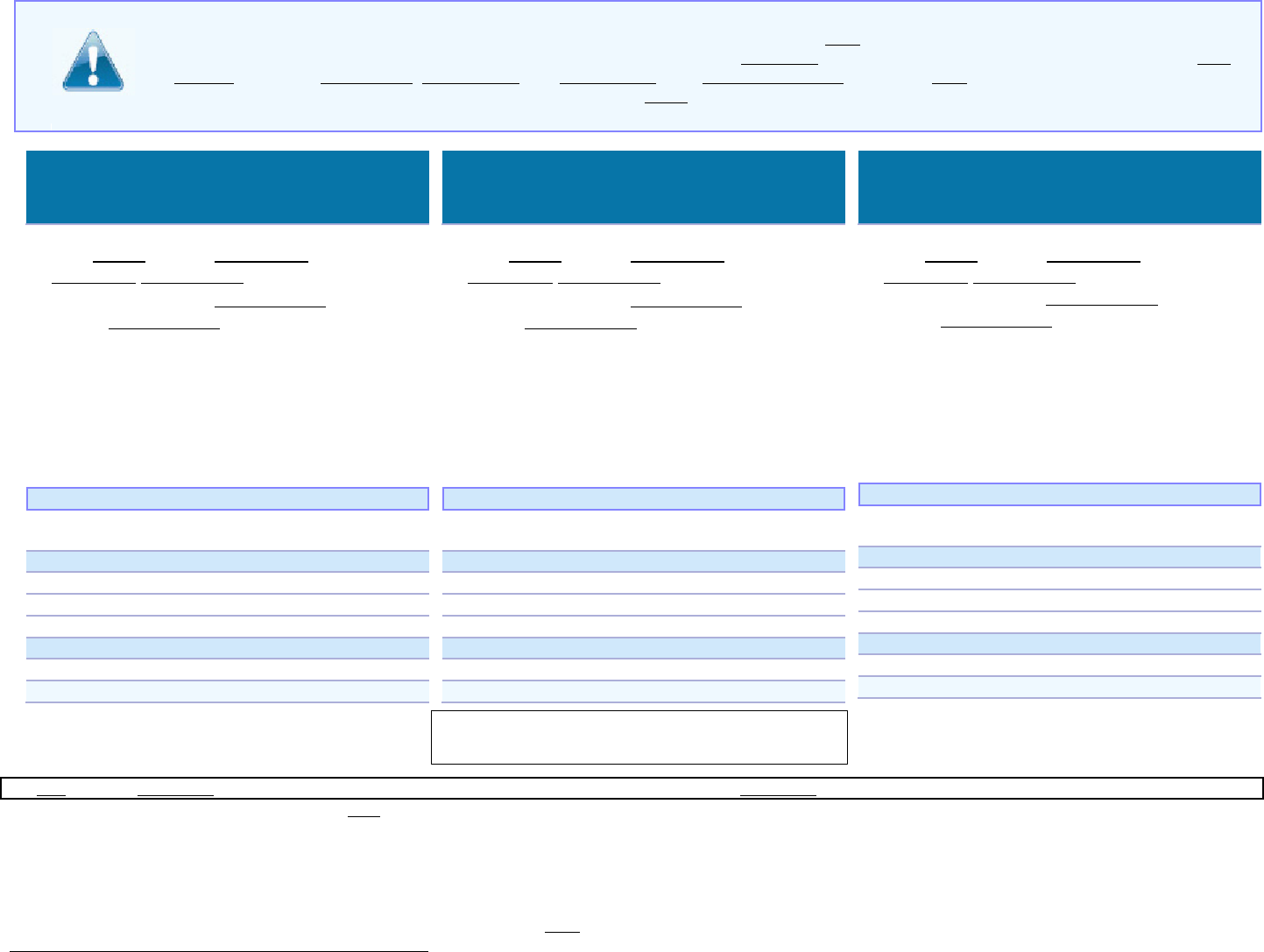
About these Coverage Examples:
This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will
be different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost
sharing amounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare
the portion of costs you might pay under different health plans. Please note these coverage examples are based on self-only coverage.
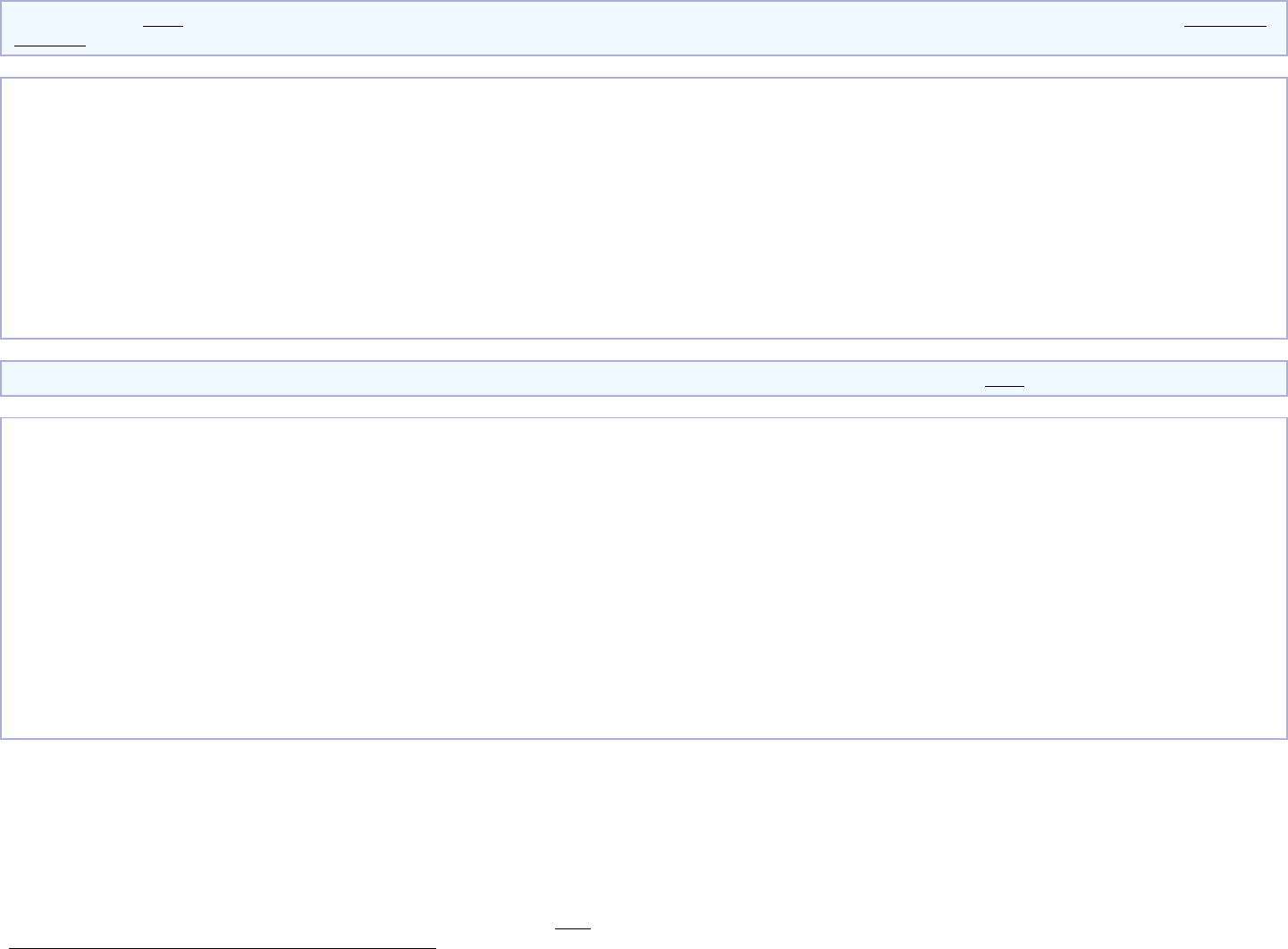
Peg is Having a Baby
(9 months of in-network pre-natal care
and a hospital delivery)
■
The plan’s overall deductible
$0.00
■
Specialist
Copayment
$15.00
■
Hospital (facility)
Coinsurance
0%
■
Other
Coinsurance
10%
This EXAMPLE event includes services like:
Specialist office visits (prenatal care)
Childbirth/Delivery Professional Services
Childbirth/Delivery Facility Services
Diagnostic tests (ultrasounds and blood work)
Specialist visit (anesthesia)
Total Example Cost
$12,700.00
In this example, Peg would pay:
Cost Sharing
Deductibles
$0.00
Copayments
$20.00
Coinsurance
$0.00
What isn’t covered
Limits or exclusions
$70.00
The total Peg would pay is
$90.00
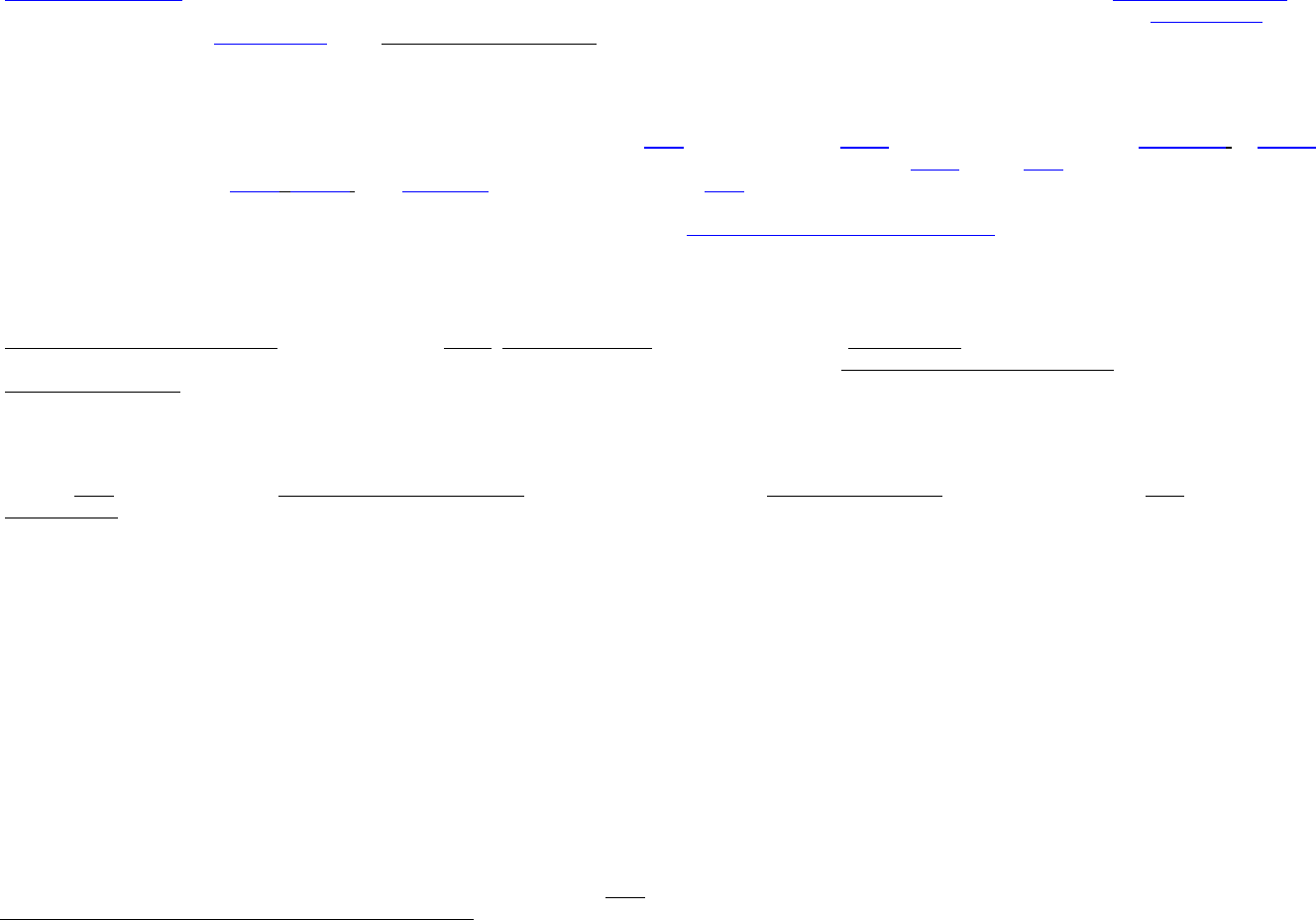
Managing Joe’s type 2 Diabetes
(a year of routine in-network care of a
well-controlled condition)
■
The plan’s overall deductible
$0.00
■
Specialist
Copayment
$15.00
■
Hospital (facility)
Coinsurance
0%
■
Other
Coinsurance
10%
This EXAMPLE event includes services like:
Primary care physician office visits (including
disease education)
Diagnostic tests (blood work)
Prescription drugs
Durable medical equipment (glucose meter)
Total Example Cost
$5,600.00
In this example, Joe would pay:
Cost Sharing
Deductibles
$0.00
Copayments
$200.00
Coinsurance
$80.00
What isn’t covered
Limits or exclusions
$3,500.00
The total Joe would pay is
$3,780.00
Mia’s Simple Fracture
(in-network emergency room visit and
follow up care)
■
The plan’s overall deductible
$0.00
■
Specialist
Copayment
$15.00
■
Hospital (facility)
Coinsurance
0%
■
Other
Coinsurance
10%
This EXAMPLE event includes services like:
Emergency room care (including medical supplies)
Diagnostic test (x-ray)
Durable medical equipment (crutches)
Rehabilitation services (physical therapy)
Total Example Cost
$2,800.00
In this example, Mia would pay:
Cost Sharing
Deductibles
$0.00
Copayments
$200.00
Coinsurance
$100.00
What isn’t covered
Limits or exclusions
$10.00
The total Mia would pay is
$310.00
This plan has other deductibles for specific services included in this coverage example. See "Are there other deductibles for specific services?" row above.
The plan would be responsible for the other costs of these EXAMPLE covered services.
Please note that some of the Limits or Exclusions listed
above may be covered under the Prescription Plan.